


Paul A. DiSilvestro, MD (Moderator)
Women’s Oncology Program Director
Rhode Island Women and Infants Hospital
Professor of Obstetrics and Gynecology
brown university
Providence, Rhode Island

event area Massachusetts, New Hampshire, Rhode Island
List of Participants Susana Campos, Maryland | Heather Benjamin, MD | Robert Koch, MD
Case summary
In August 2021, a 64-year-old postmenopausal woman complained of abnormal uterine bleeding that had lasted for 4 months. She had a history of arthritis, obesity (BMI = 40), and well-controlled hypertension. Her ECOG performance status was her 1. She was counseled about her surgical options and scheduled for surgery. She was diagnosed with stage IA, grade 1 endometrial cancer. Immunohistochemistry and molecular testing showed the disease to be mismatch repair deficient (dMMR), high microsatellite instability (MSI-H), and 3+ estrogen receptor positivity.
In August 2022, she reported intermittent pelvic pain for the past 4 weeks. Her CT scan (CT CAP) of her chest, abdomen, and pelvis suggested recurrent/metastatic disease with involvement of one right external iliac lymph node. Carboplatin/paclitaxel was administered to her every 4 weeks for 6 cycles. Chemotherapy was well tolerated, with a complete response (CR) recorded at the end of therapy.
In April 2023, a recurrence of the disease was recorded during routine follow-up. CT CAP showed a heterogeneously enhancing mass in the right suprarenal space, multiple bilateral pulmonary nodules, and a new right internal iliac lymph node in addition to the previously observed positive lymph nodes. Fine needle aspiration of the renal accessory mass confirmed metastatic endometrioid adenocarcinoma. Patients were counseled about systemic therapy options, during which they repeatedly expressed concerns about adverse events (AEs).
Latest information on the incident
Through shared decision-making, immune checkpoint inhibitor (ICI) monotherapy was planned. The patient was started on dostarlimab (Gemperi) with instructions to continue follow-up every 3 months.
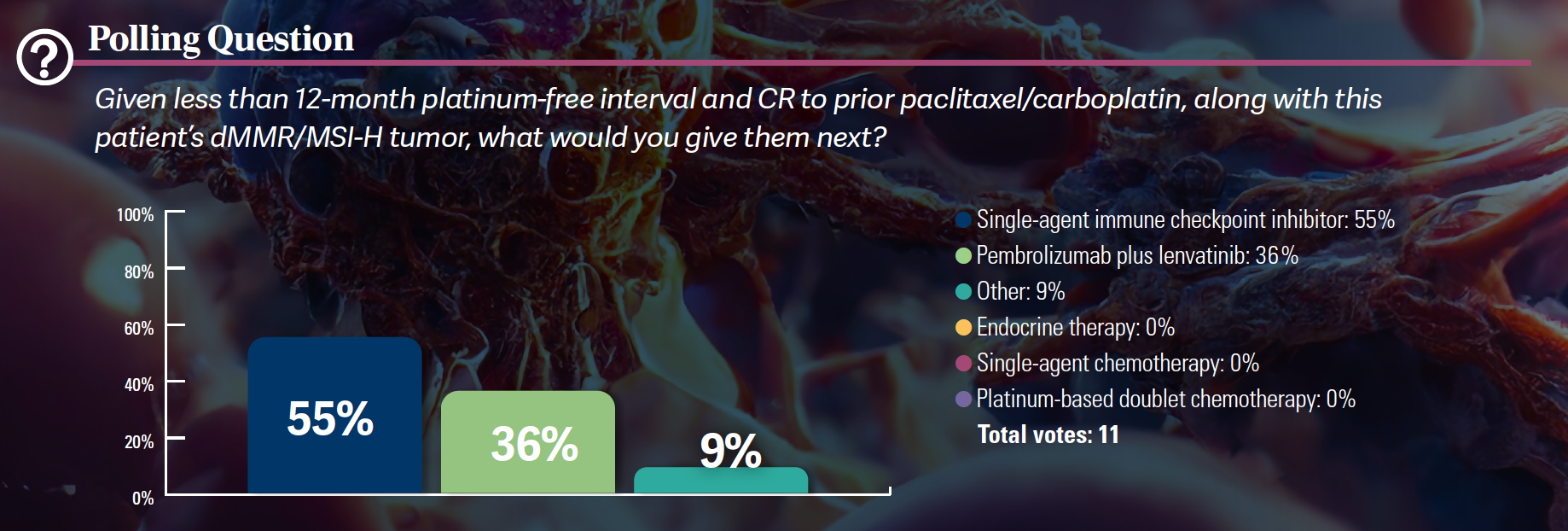
discussion questions
- What factors influence the preference for immune checkpoint inhibitors in these patients?
Di Silvestro: When considering teaching residents, peers, and yourself. Say, “We have this. [patient with] dMMR Recurrent endometrial cancer. She wants to give her her ICI, but how do she decide which of the two to choose? [treatments]? ” What factors do you consider when choosing one?
Campos: I wish I could influence it, but it’s essentially influenced by our pharmacy.
Di Silvestro: That’s a great point.We are very active at GARNET [NCT02715284] and ruby [NCT03981796] And I went to the pharmacy and said I want to order dostarlimab for this patient.They are [said] They officially don’t have it.I 1699200059 Now that I finally understand, Dr. Campos, you are absolutely right. What’s in the official collection? [Do you have] Pembrolizumab [Keytruda]?
Campos: There’s pembrolizumab. That’s interesting, and this might be a point for us to discuss…the endpoints of the particular study and what those endpoints were, and any impact those endpoints have on what the formulary should have. This is from the perspective of whether or not to give.
If there is an overall survival benefit, it should be prioritized [another study with] Is there no survival benefit? I think these are great questions that will come to light. We have pembrolizumab and we introduced dostarlimab. It was a very thoughtful process in terms of yes and no, but at the end of the day, are these things really in our control?
Di Silvestro: Other experience [participants] Don’t pharmacies allow both?
Benjamin: we were initially [only] Pembrolizumab was approved because there are multiple sites of disease that we advocate for. [for dostarlimab], there are various malignancies such as rectal cancer, so it was difficult for the administration to say no, as it had to be added to the prescription. Fortunately, we were able to do the following: [get it]but I agree, everything takes time and effort and you have to prove why it’s needed.
Koch: This patient has lung metastasis and has an incurable disease. I didn’t really understand what her symptom burden was, which made it a little harder to make choices for her. Given the fact that she has an incurable disease, that needs to be factored into the decision-making process, and it is my understanding that dostarlimab is an expensive long-term treatment. We do not know if the quality of life of these patients will improve. That’s why, [would] Choose pembrolizumab.
Di Silvestro: That’s a great point. I am on dostarlimab…and that is primarily because I am participating in a clinical trial that uses dostarlimab.I can not do it [dismiss] Some say one is more effective than the other, but that was well known to us. We did not participate in the KEYNOTE study. There are many reasons to choose one or the other.Dosage and schedule [are a factor]; obviously, you can now move on to a 6-weekly strategy [for pembrolizumab]it’s also the same [for dostarlimab after 4 doses]. Pharmaceutical reimbursement is an important point brought up by Dr. Koch.
moderator sidebar
Q: What is the most noteworthy aspect of dostarlimab in terms of safety as a single agent?
Di Silvestro: Looking at the GARNET trial [NCT02715284]Ninety-nine percent of patients experienced some type of treatment-emergent AE, and 58% experienced some form of grade 3 AE.1 Although multiple grade 3 events may have occurred in a single patient, the rate of grade 3 treatment-related AEs was approximately 19% in the overall population. Less than half of these were due to possible immune-related treatment-related AEs. Most of the AEs that occurred during treatment were grade 1 or 2 and manageable, as no patient died. This led to about 9% of patients discontinuing treatment, about half of what was seen in the RUBY trial. [NCT03981796] for dostarlimab [plus chemotherapy].2 GARNET has a lower percentage. …Treatment-related AEs are seen with hepatitis and diarrhea reflecting colitis, hyperglycemia, and pneumonia. These AE types are reviewed in our article. [practice].
discussion questions
- Please share your experience with immune-related AEs in patients receiving ICI-based regimens for endometrial cancer.
- What are the strategies for mitigating or managing AEs?
Di Silvestro: do [you] Wait for free T4 level response and restart ICI treatment, or [would] Just start levothyroxine and hold down [From the Data1,3]?
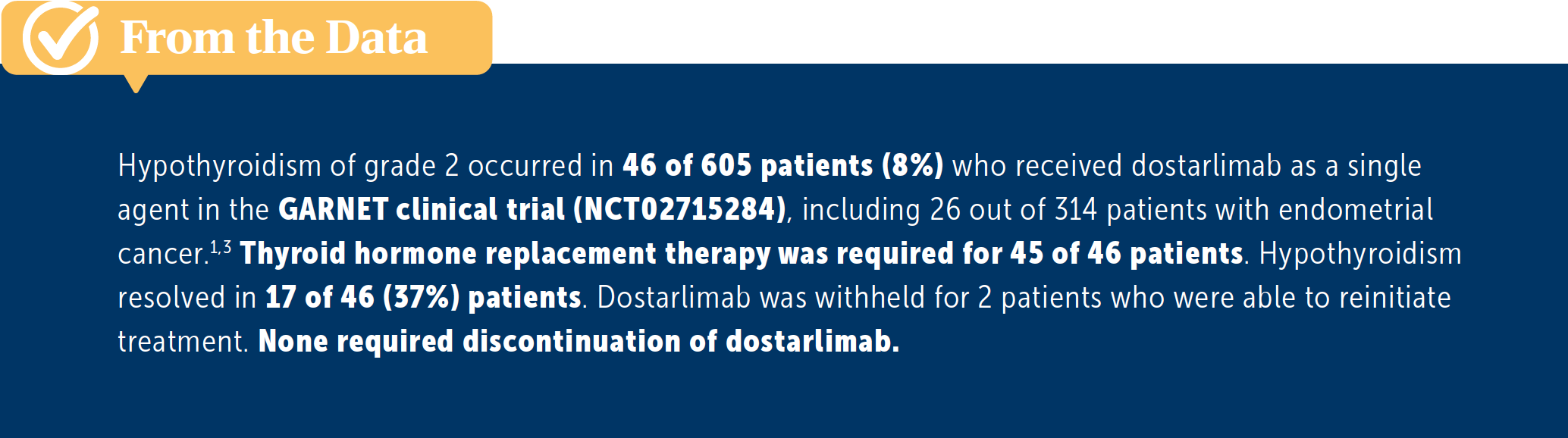
Benjamin: Because this patient was symptomatic, he is warned to restart and start levothyroxine at the same time, a decision that may be forthcoming in some patients. It is rather an abnormality seen in the laboratory.It’s not extreme and those are the patients I need more of [likely] Consider coadministration with levothyroxine while waiting for normalization.But based on the symptoms, I’m hoping until its normalization, or at least [until] Things are improving and the symptoms are gone.
Di Silvestro: Yes, and in so many cases of these patients, we’re just seeing it from the serum panel, and for so many people, we’re seeing it as a lab abnormality, and they’re not affected, but , and eventually begin treatment. For this group as a whole, from what you see in clinical trials, does your real-life experience reflect what you’ve seen in these trials? Are you seeing anything unusual? More than what the trials show? Do you see things happening at a high rate, or does it seem consistent?
Campos: everyone knows [about] pneumonia, colitis, [and] hepatitis.It’s more of a subtle issue that you don’t know about. [about]. I had a patient with hypercalcemia that was ultimately related to pembrolizumab, and we treated her based on some case reports, but I don’t think that’s what arose from that. Masu. That’s not a common thing we’ve all heard. It could be that the test results are… abnormal, and you… I don’t know if that makes sense, but it could essentially be related to a system that you haven’t thought about enough. It’s a subtle thing that there isn’t. The part I’m most worried about is [an ICI] Anything can happen, so when you see something, you have to think it could be related to pembrolizumab or dostarlimab or some other unspecified immunotherapy.The most difficult thing is knowing when to act or [not], and if you act, will you be denying what you were trying to achieve? This is the part that becomes. [challenging when] Deal with these types of agents.
Di Silvestro: Well, to your point, I know there are certain facilities that have teams that intervene in AEs related to immune checkpoint inhibition. There are some general guidelines, but [ for example, from] American Society of Clinical OncologyFour….There are very specific guidelines on how to do this, and resources can be found in many places. What’s interesting about ICIs is that there are no recommendations for reducing the dose.
Campos: right.
Di Silvestro: People here have managed ICI before, but we’ve also seen some pretty serious cases. [AEs]. I’ve seen some very severe cases of colitis, which is unfortunate.
Campos: In the past, I have seen people die from toxicity from early immunotherapy treatments. These are very interesting drugs that sometimes take unpredictable directions.
Benjamin: flat [with] Atypical Symptoms – A lung cancer patient I worked with who first received chemoradiotherapy and then immunotherapy had some difficulty swallowing during the immunotherapy.i was thinking [about the] He underwent chemoradiotherapy and an endoscopy to try to find the cause, but it was ultimately determined that his main focal symptom was myasthenia gravis, which was related to the immunotherapy. [was] Difficulty swallowing.
It didn’t cross my mind for a while. He had difficulty for several weeks and his symptoms progressed to the point that he was hospitalized and was no longer able to take oral intake. In that sense, it was quite unusual. [it is] Things to consider [with] wider differential [as to] you [should] Do you think it is related to ICI?
Campos: I [suspect] Immunotherapy for everyone [AE] Until proven otherwise.
Koch: All you need to know is Phase 1 [data] In immunotherapy, it is used to determine which doses are proven to be effective and safe. I don’t know those data, but I don’t think there are any guidelines to reduce the dose because the doses we’re used to are those based on previous trials and studies that have proven to be effective. Masu. safety. I think these are noteworthy data.
Di Silvestro: No, I think so too. This is a question of safe doses of exposure, not how much you ingest. Is it effective, whether you can get it, whether we can drop it? I don’t have that data either.
References:
1. Oknin A, Gilbert L, Tinker AV, et al. Safety and antitumor activity of dostarlimab in patients with advanced or recurrent DNA mismatch repair deficiency/microsatellite instability-high (dMMR/MSI-H) or high/stable (MMRp/MSS) endometrial cancer: GARNET -a Phase I, interim results of a single agent-arm study. J Immune Cancer. 2022;10(1):e003777. doi:10.1136/jitc-2021-003777
2. Mirza MR, Chase DM, Slomowitz BM, et al. Dostarlimab for primary advanced or recurrent endometrial cancer. N English J Medicine. 2023;388(23):2145-2158. doi:10.1056/NEJMoa2216334
3. Gemperi. Prescription information. GlaxoSmithKline; 2023. Accessed September 19, 2023. https://tinyurl.com/ym67vkm6
4. Schneider BJ, Naidu J, Santomaso BD, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: An update to the ASCO guidelines. J Clin Oncor. 2021;39(36):4073-4126. doi:10.1200/JCO.21.01440