

 | BMC Medicine")
Participant characteristics
The study included 6,800 patients diagnosed with primary brain tumors in Wales between 2000 and 2014, and 33,785 controls matched on age, gender and GP practice. Cohort selection is shown in Figure 1. The total follow-up time for brain tumor patients and their controls was 32,453.9 person-years (median 3.5 years, interquartile range). [IQR] 3.5–10.1) and 247,142.1 person-years (median 6.6 years, IQR 3.9–10.3). There were 2,869 patients with malignant tumors, of whom 1,340 (46.1%) had glioblastoma. Of the 3,931 patients with non-malignant tumors, 1,498 (38.1%) had non-malignant meningiomas. Characteristics of the study cohort are shown in Table 1. Characteristics of the corresponding cohorts of glioblastoma and meningioma are shown in Additional file 1: Table S1. Primary treatment data are available in Table S2 in Additional file 1.
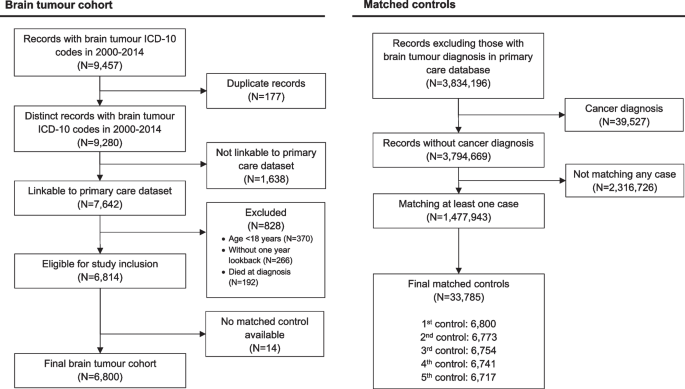
Cohort selection for this matched cohort study of people who participated in the SAIL databank in Wales (UK) between 2000 and 2014. The study included 6,800 of 6,814 (99.8%) eligible patients diagnosed with malignant or non-malignant tumors. Of 1,477,932 eligible controls, 33,765 (2.3%) were included as matched controls. The control group had not been diagnosed with cancer and were matched on date of birth within the past five years, gender, and medical history from a general practitioner.
Malignant tumor
Of the 2,869 patients with malignancy, 252 (8.8%) patients experienced at least one cardiovascular event within 1 year of diagnosis. There were 89 patients with major vascular events and 170 patients with VTE (Figure 2). The crude incidence rates per 1000 person-years in the first year for patients with malignant brain tumors and their controls were 54.1 (95% CI 43.4 to 66.6) for major vascular outcomes and 48.1 (95% CI 44.5 to 52.0) for major vascular outcomes; For vascular outcome it was 106.7 (95% CI). For VTE, they were % CI 91.3 to 124.0) and 4.9 (95% CI 3.8 to 6.2), respectively. In a fully adjusted Cox model, malignant brain tumor was associated with his VTE (hazard ratio). [HR] 21.58, 95% CI 16.12–28.88, p< 0.001), hemorrhagic stroke (HR 6.63, 95% CI 3.75 to 11.70; p< 0.001), ischemic stroke (HR 1.88, 95% 95% CI 1.06-3.36, p= 0.032) but not IHD (HR 0.67, 95% CI 0.45 to 1.00, p= 0.051) or aortic and peripheral vascular disease (HR 1.17, 95% CI 0.56 to 2.47; p= 0.674). In multivariate analysis of patients with 1-year survival compared to controls, malignant brain tumor diagnosis was associated with VTE (HR 2.20, 95% CI 1.52-3.18; p< 0.001) and all stroke types combined (HR 1.45, 95% CI 1.00 to 2.10; p= 0.047) (Figure 2). 1-year survivors had a lower risk of her IHD compared to controls (HR 0.58, 95% CI 0.37–0.89, p= 0.013).
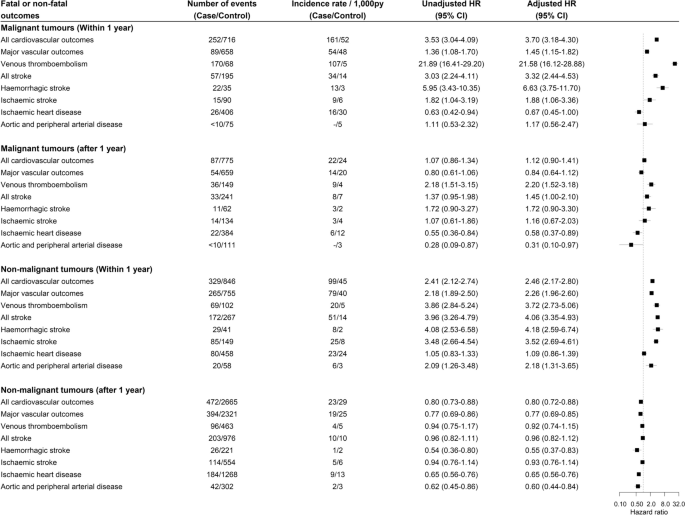
Crude incidence and hazard ratios of cardiovascular events after tumor diagnosis in people diagnosed with malignant or non-malignant brain tumors compared with matched controls.Diagnosis of brain tumor, Welsh index of multiple blockade, heavy alcohol use, hypercholesterolemia, past major vascular events, past venous thromboembolism, use of antiplatelets, use of anticoagulants, use of antihypertensive drugs, Multivariate Cox regression adjusted for age and gender
non-malignant tumor
Of the 3,931 patients with non-malignant tumors, 329 (8.4%) experienced at least one cardiovascular event within 1 year of diagnosis. There were 265 patients with major vascular events and 96 patients with VTE (Figure 2). The incidence rates per 1000 person-years in the first year for patients with non-malignant tumors and their controls were 78.8 (95% CI 69.6 to 88.8) for major vascular outcomes, 40.3 (95% CI 37.5 to 43.3) and 20.0 (for VTE). were 95% CI 15.5 to 25.3) and 5.4 (95% CI 4.4 to 6.5), respectively. In multivariate analysis, non-malignant tumor diagnosis was associated with VTE (HR 3.72, 95% CI 2.73 to 5.06; p< 0.001), hemorrhagic stroke (HR 4.18, 95% CI 2.59 to 6.74; p< 0.001), ischemic stroke (HR 3.52, 95% CI 2.69 to 4.61, p< 0.001) and aortic and peripheral artery disease (HR 2.09, 95% CI 1.26 to 3.48, p= 0.003). In patients who survived 1 year after tumor diagnosis, non-malignant tumors were associated with a lower risk of hemorrhagic stroke compared with controls (HR 0.55, 95% CI 0.37 to 0.83; p= 0.004), ischemic heart disease (HR 0.65, 95% CI 0.56 to 0.76, p< 0.001) and aortic and peripheral artery disease (HR 0.60, 95% CI 0.44 to 0.84, p= 0.003) (Figure 2).
Tumor subgroup
There were 1,340 patients with glioblastoma (Additional file 1: Table S1), and 137 (10.2%) of these patients had at least one cardiovascular event within 1 year of diagnosis. Major vascular events occurred in 36 (2.7%) patients and her VTE occurred in 107 (8.0%) patients (Additional file 1: Figure S2). The incidence rates per 1000 person-years in first-year glioblastoma patients and controls were 50.7 (95% CI 35.5 to 70.3), 52.6 (95% CI 47.1 to 58.6), and 159.4 (95 %CI 130.6~). for VTE they were 192.6) and 4.7 (95% CI 3.2-6.8), respectively. In the adjusted Cox model, glioblastoma diagnosis was associated with VTE (HR 31.78, 95% CI 20.99 to 48.13; p< 0.001) and hemorrhagic stroke (HR 5.02, 95% CI 2.16 to 11.67, p< 0.001) (Additional file 1: Figure S2). We did not investigate these associations in patients who survived 1 year due to the small number of observed outcomes. There were 291 glioblastoma patients who survived 1 year without cardiovascular events, but 15 of them developed CVD during the remaining follow-up period.
Of the 1,498 meningioma patients (Additional file 1: Table S1), 184 (12.3%) experienced at least one cardiovascular event within 1 year of diagnosis. Major vascular events and VTE occurred in 162 (10.8%) and 36 (2.4%) patients, respectively. The incidence rates per 1000 person-years in meningioma patients and their controls were 123.6 (95% CI 104.7 to 145.0) and 52.0 (95% CI 46.8 to 57.7) and 29.6 (95% CI 20.9 to 40.6) and 4.9. (95% CI 3.4 to 6.8). In a multivariate model, meningioma diagnosis was associated with VTE (HR 5.90, 95% CI 3.71 to 9.38; p< 0.001), hemorrhagic stroke (HR 3.80, 95% CI 2.01-7.18, p< 0.001) and ischemic stroke (HR 4.37, 95% CI 3.09 to 6.18, p< 0.001). Meningioma patients surviving 1 year after tumor diagnosis had a lower risk of hemorrhagic stroke (HR 0.37, 95% CI 0.17 to 0.80; p= 0.011), ischemic heart disease (HR 0.72, 95% CI 0.55 to 0.93, p= 0.013), aortic and peripheral artery disease (HR 0.45, 95% CI 0.23 to 0.86, p= 0.015) (Additional file 1: Figure S2).
Incidence of cardiovascular events in the first year of diagnosis
A multivariable flexible parametric model was used to estimate the incidence of major vascular events and VTE in tumor groups stratified by age (Figure 3). The incidence of VTE showed a bimodal distribution, with peaks at 1 and 5 months for malignancies. People with non-malignant tumors had the highest incidence of major vascular events early after tumor diagnosis. Patients who underwent surgery for malignant brain tumors had the highest risk of her VTE at 1 and 5 months after diagnosis, whereas this was not observed in patients who did not undergo surgery (Additional file 1: Figure S3). Trends in outcome events for patients with malignancy stratified by surgical status were similar to the overall trends.
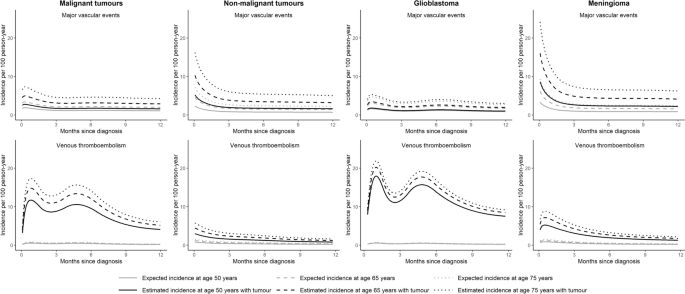
Incidence of major vascular and venous thromboembolic events within 1 year of study entry. We consider brain tumor diagnosis, Welsh index of multiple blockade, heavy alcohol use, hypercholesterolemia, past major vascular events, past venous thromboembolism, antiplatelet use, anticoagulant use, and antihypertensive medications. We used a flexible parametric survival model with four degrees of freedom adjusted for age and sex. Estimate the incidence of CVD. Predicted incidence rates at ages 50, 65, and 75 were generated.
Sensitivity analysis
Analyzes using multivariable Cox models, including BMI and smoking status, showed similar results to the main analysis (Additional file 1: Figure S4). Brain tumor patients who had a stroke within his 14 days were excluded because the majority of strokes occurred soon after tumor diagnosis. Patients with malignant tumors who survived 14 days without stroke had a higher risk of all types of stroke (including unspecified stroke) and hemorrhagic stroke (Additional file 1: Figure S5). Non-malignant tumor patients who survived 14 days without a stroke had an increased risk of all stroke subtypes (Additional file 1: Figure S6). The direction of the subhazard ratios in the competing risks analysis was consistent with the cause-specific analyzes shown in Figures 2 and 3. 2 and 3 (Additional file 1: Tables S3 and S4).
Antiplatelet drug use and cardiovascular disease outcomes
The absolute number of patients with cardiovascular disease within 1 year after diagnosis is shown in Table 2 by tumor type, surgical status, and antiplatelet drug use. Some numbers are not shown due to data suppression to minimize disclosure risk. Across the patient population, with the exception of meningioma patients who did not undergo surgery, a higher proportion of patients who were taking antiplatelet drugs at diagnosis had a major vascular event.